The Democratic Republic of the Congo is facing a rapidly escalating medical emergency as confirmed Ebola cases have officially surged to 282. The outbreak, centered in the volatile eastern Ituri province, has also generated more than 1,000 suspected cases and claimed 42 confirmed lives. While international headlines focus on the emotional triumphs of the few health workers who have survived, a far grimmer reality is unfolding on the ground. Health officials are privately terrified because this epidemic is driven by the Bundibugyo virus, a rare species of Ebola for which there is no approved vaccine and no proven therapeutic treatment.
Public health infrastructure in eastern Congo is buckling under a crisis that standard protocols cannot contain. The boilerplate optimism offered by visiting dignitaries masks a structural collapse in containment strategies. With a contact tracing coverage rate stalled at a dismal 45%, the virus is moving faster than the teams assigned to track it.
The Illusion of Victory in Bunia
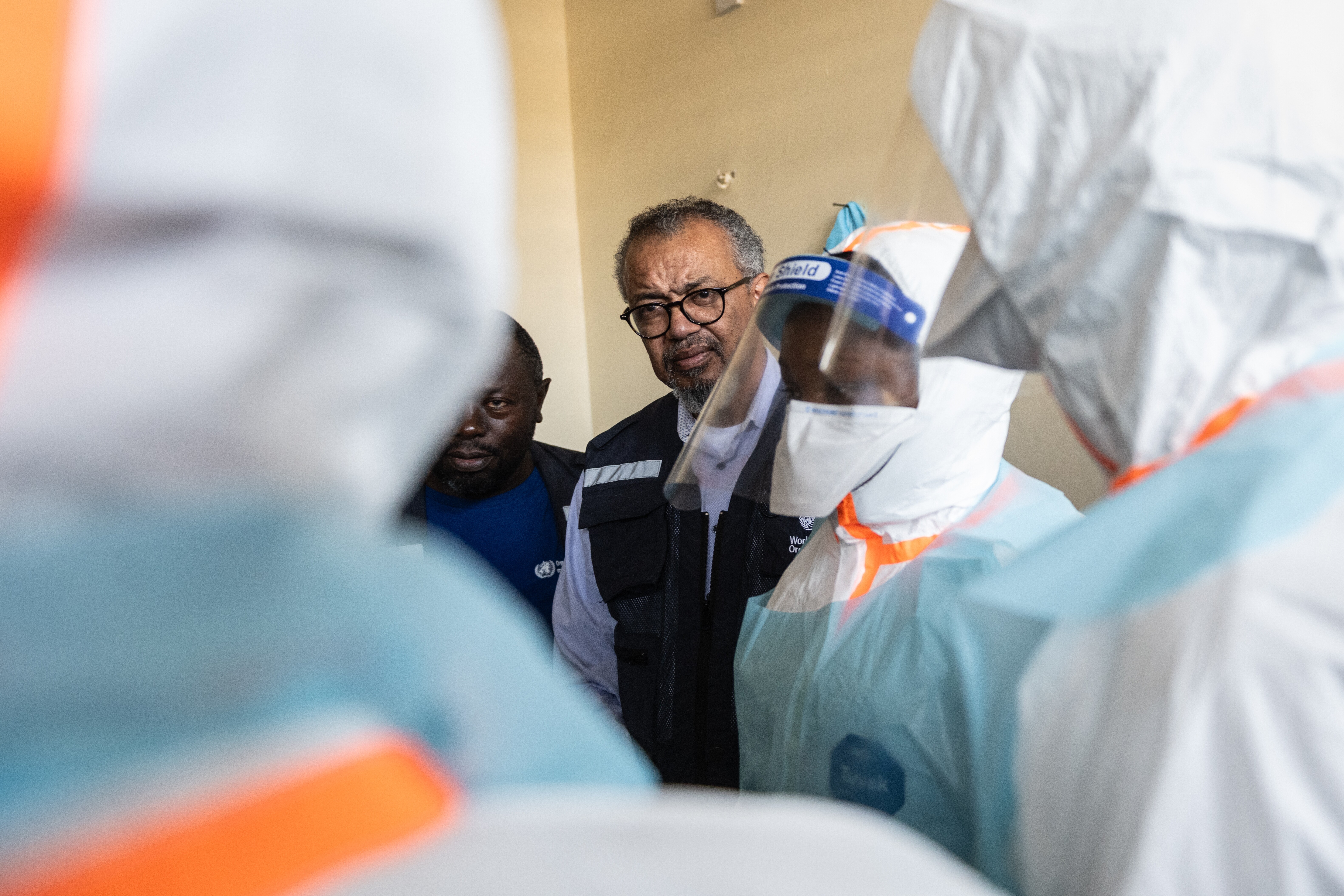
Over the weekend, World Health Organization Director-General Tedros Adhanom Ghebreyesus arrived in Bunia, the capital of Ituri province, to inaugurate a new Ebola treatment center. The event featured the presentation of recovery certificates to five individuals, all of them frontline medical workers. Among them were Baraka Bulambulu and Ezo Étienne, nurses who contracted the virus while tending to patients.
Their survival is a testament to individual resilience and aggressive supportive care, but using these rare success stories to project a turning point in the crisis is deeply misleading. Five recoveries against a backdrop of nearly 300 confirmed cases and over a thousand suspected infections is not a winning ratio. It is a statistical anomaly.
The Vulnerability of the Front Line
The fact that all five initial survivors are medical professionals highlights a systemic failure in basic infection prevention. When an outbreak hits an area with underfunded clinics, the healers quickly become the vectors.
- Ezo Étienne's Collapse: Étienne was conducting routine ward rounds when sudden hypotension and violent vomiting signaled his infection.
- The Transmission Loop: Without adequate personal protective equipment (PPE), a single undiagnosed patient in a general ward can infect an entire shift of nurses.
- The Trust Deficit: When the local population sees doctors and nurses dying in the fields, faith in Western medicine evaporates, driving infected individuals underground.
Why the Bundibugyo Strain Changes Everything
To understand why this specific outbreak is causing panic in Geneva and Kinshasa, one must look at the virology. Most recent, highly publicized Ebola interventions relied heavily on the Ervebo vaccine and monoclonal antibody treatments like Ebanga and Inmazeb. Those medical breakthroughs, however, were engineered exclusively to fight the Zaire strain of the virus.
Against the Bundibugyo species, those tools are entirely useless.
Medical teams are forced to rely on sympathomimetic support, intravenous fluids, and electrolyte replacement. They are essentially fighting a medieval war with modern telemetry. If a patient’s immune system cannot mount a defense on its own, supportive therapy only delays the inevitable. This lack of pharmaceutical armor makes early detection and rapid isolation the only viable defense mechanics, both of which are currently failing in Ituri.
The Breakdown of Containment Mechanics
Congo's Ministry of Health recently outlined the primary pillars required to blunt the momentum of the virus. They include rigorous contact tracing, early isolation, and safe, dignified burials. None of these pillars are currently stable.
| Containment Pillar | Required Target | Current Metric | Impact on Outbreak |
|---|---|---|---|
| Contact Tracing | > 90% coverage | 45% coverage | More than half of all potential exposures are unmonitored, allowing the virus to seed new community clusters undetected. |
| Suspected Case Isolation | Immediate | 220 pending | Delays in laboratory turnarounds mean suspected patients remain in community settings or general clinics, compounding exposure risk. |
| Border Biosecurity | Sealed corridors | Active panic | Uganda has closed its borders after recording nine cases, while local protests in neighboring Kenya against quarantine facilities demonstrate regional instability. |
The math is simple and unforgiving. When contact tracing drops below 50%, the chain of transmission becomes completely invisible. Field epidemiologists are no longer managing an outbreak; they are chasing a ghost.
Geography and Violence as Viral Allies
The epicenter of this crisis is not just remote; it is actively hostile. Eastern Congo has been plagued by decades of armed conflict involving dozens of rebel militias.
Epidemiology requires stability. You cannot track a contact through a village that has been abandoned due to an insurgent raid. You cannot safely transport blood samples down roads controlled by armed syndicates.
"The intersection of a rare pathogen and active warfare creates a worst-case scenario for field medicine. The traditional playbook assumes cooperation and physical access, neither of which can be guaranteed in Ituri."
💡 You might also like: Why RFK Jr Is Calling Out Dunkin Iced Coffee
Whenever violence flares, field teams are pulled back, isolation protocols are broken, and the virus gains weeks of uncontested ground. The current spread into North Kivu (15 cases) and South Kivu (3 cases) proves that regional containment has already failed.
The Threat of Regional Contagion
The anxiety is no longer confined to the borders of the Congo. Uganda's swift decision to close its border came after nine confirmed cases appeared within its territory, resulting in at least one death.
Further east, the geopolitical ripples are turning into public protests. In Laikipia, Kenya, hundreds of youths recently demonstrated against the proposed establishment of an Ebola quarantine center intended for affected U.S. citizens at a local air base. Governor Joshua Irungu publicly backed the protestors, warning that housing infected individuals locally would expose the domestic population to a strain they are entirely unprepared to handle.
This panic is a direct consequence of the regulatory vacuum surrounding the Bundibugyo strain. International partners cannot fly in millions of vaccine doses because those doses do not exist. The global community is realizing that a major outbreak of an untreatable sub-species cannot be managed by public relations campaigns or celebratory photo-ops in Bunia. It requires an immediate, massive deployment of field hospitals, raw containment infrastructure, and an acceptance that the current containment strategy is fundamentally broken.



